Prostate Cancer Overdiagnosis: Navigating the Hidden Epidemic
Imagine being told you have cancer, undergoing invasive treatments, and dealing with side effects—only to later learn that your cancer would never have caused symptoms or threatened your life. This is the reality for many men diagnosed with prostate cancer today. It highlights a significant yet often overlooked issue in modern medicine: the overdiagnosis of prostate cancer.
Understanding Overdiagnosis
Overdiagnosis happens when a disease is diagnosed that would not have caused symptoms or death during a person's lifetime. In prostate cancer, this is particularly common due to the widespread use of the prostate-specific antigen (PSA) test. PSA is a protein produced by both normal and cancerous cells of the prostate gland. High PSA levels can signal cancer, but can also result from non-cancerous conditions like prostatitis (inflammation of the prostate) or benign prostatic hyperplasia (BPH), which is an enlarged prostate. The challenge is telling apart aggressive tumors that need treatment from slow-growing ones that don't.
The Rise of PSA Screening and Its Implications
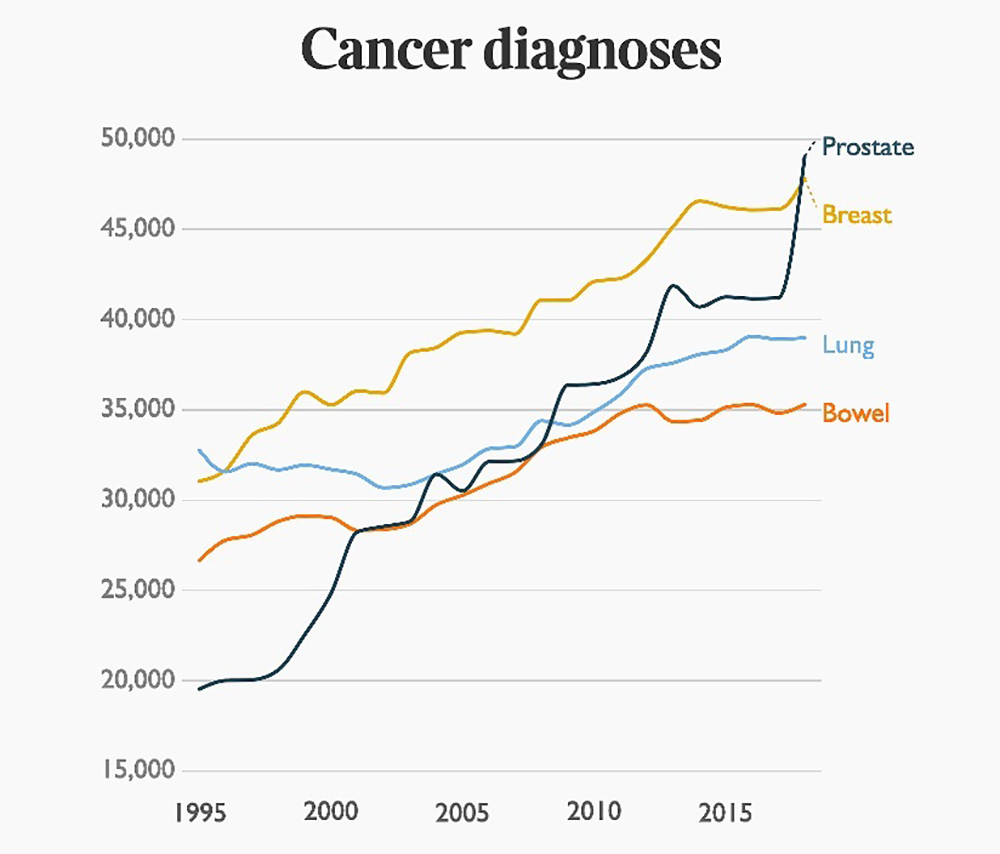
In the late 1980s and early 1990s, PSA testing became a common way to detect prostate cancer early. While this led to more cases being diagnosed, it also brought attention to the critical issue of overdiagnosis.
A major study published in the New England Journal of Medicine looked at the European Randomized Study of Screening for Prostate Cancer (ERSPC), involving over 182,000 men aged 50 to 74 across eight European countries. After nine years, the study found that PSA screening reduced prostate cancer deaths by about 20%. However, to prevent one prostate cancer death, 1,410 men needed to be screened, and an additional 48 men would need to be treated[1]. This means many men were diagnosed and possibly treated for cancers that might not have caused harm if left undetected.
Similarly, the Prostate, Lung, Colorectal, and Ovarian (PLCO) Cancer Screening Trial in the United States studied the effect of yearly PSA testing and digital rectal exams on prostate cancer deaths. The initial results, after seven years, showed no significant reduction in prostate cancer deaths between the screening group and the control group [2].
An extended follow-up study published in 2012 provided results after 13 years. This study still showed no significant mortality benefit from regular annual screening compared to usual care [3]. Specifically, the rate ratio for prostate cancer deaths was 1.09 (meaning a 9% increase, but not statistically significant), indicating no clear difference between the groups.
Also, the number of prostate cancer cases remained significantly higher in the screening group, suggesting overdiagnosis. Over the extended follow-up, there were 108.4 prostate cancer cases per 10,000 person-years in the screening group compared to 97.1 per 10,000 person-years in the control group. This represents a 12% relative increase in prostate cancer diagnoses in the screening group (rate ratio of 1.12) [3].
Consequences of Overdiagnosis and Overtreatment
Overdiagnosis often leads to overtreatment, where men undergo unnecessary procedures and face associated risks. Treatments like radical prostatectomy (surgical removal of the prostate) and radiation therapy can have significant side effects, including:
- Urinary incontinence (loss of bladder control)
- Erectile dysfunction (difficulty achieving or maintaining an erection)
- Bowel problems, such as diarrhea or rectal bleeding
The ProtecT trial, a landmark study published in the New England Journal of Medicine, compared active monitoring (watching the cancer closely), surgery, and radiotherapy in men with localized prostate cancer [4]. After ten years, there were no significant differences in prostate cancer deaths among the groups. However, those who had surgery or radiotherapy experienced higher rates of side effects compared to those under active monitoring. This finding shows that immediate aggressive treatment may not always be necessary and can negatively affect quality of life.
Moreover, being diagnosed with cancer can have a significant psychological impact. Anxiety, depression, and reduced well-being are common among men diagnosed with prostate cancer, even when the cancer is unlikely to progress.
Strategies to Reduce Overdiagnosis
Recognizing the challenges of overdiagnosis, the medical community has explored ways to reduce unnecessary detection and treatment of slow-growing prostate cancers.
Risk Stratification Tools
Advancements in diagnostic tools aim to improve the accuracy of prostate cancer screening. For example, the Prostate Health Index (PHI) and 4Kscore tests combine multiple biomarkers to better predict the risk of aggressive prostate cancer. Studies have shown that these tests are better than PSA alone at identifying significant cancers, potentially reducing unnecessary biopsies [5].
Multiparametric MRI
Using multiparametric magnetic resonance imaging (mpMRI) before a biopsy has greatly improved the detection of significant prostate cancers while reducing the identification of insignificant ones. A 2018 study showed that using mpMRI to guide biopsies led to fewer men being diagnosed with low-risk cancer and more men being diagnosed with high-risk cancer compared to standard biopsy methods [6].
Active Surveillance
Active surveillance means closely monitoring prostate cancer with regular PSA tests, physical exams, and repeat biopsies, and starting treatment only if the cancer shows signs of getting worse. This approach balances the need to treat aggressive cancers quickly while avoiding overtreatment of slow-growing ones.
Long-term studies have confirmed the safety of active surveillance for low-risk prostate cancer. A study in the Journal of Clinical Oncology reported that after an average follow-up of 6.4 years, the prostate cancer-specific survival rate was 99.7% among men managed with active surveillance [7]. This suggests many men can safely delay or avoid treatment without risking their survival. The study concluded that "active surveillance for favorable-risk prostate cancer is feasible and seems safe in the 15-year time frame."
Guideline Recommendations
Medical organizations have updated their guidelines to reflect these advancements.
- The American Urological Association (AUA) recommends shared decision-making for PSA screening in men aged 55 to 69. This means doctors and patients should discuss the pros and cons, considering what's important to the patient [8].
- The U.S. Preventive Services Task Force (USPSTF) makes a similar recommendation. They highlight that the decision to have PSA-based screening should be an individual one, made after discussing potential benefits and harms with a doctor. They note that "screening offers a small potential benefit of reducing the chance of death from prostate cancer in some men" [9].
The USPSTF further states, "Many men will experience potential harms of screening, including false-positive results that require additional testing and possible prostate biopsy; overdiagnosis and overtreatment; and treatment complications, such as incontinence and erectile dysfunction" [9].
Shared Decision-Making: Empowering Patients
Shared decision-making is a collaborative process where patients and healthcare providers make health decisions together. It considers the best scientific evidence available, along with the patient's values, preferences, and circumstances.
In prostate cancer screening, shared decision-making involves discussing:
- Potential benefits of screening like early detection of aggressive cancers.
- Risks of overdiagnosis and overtreatment, including side effects from unnecessary treatments.
- Alternative strategies, such as active surveillance, may be suitable for some patients.
By having open and honest conversations, doctors can help patients make informed choices that align with their personal health goals.
Natural Supplements for Prostate Health
Emerging research suggests that certain natural supplements may support prostate health and potentially help lower PSA levels.
Beta-sitosterol and Saw Palmetto
Beta-sitosterol and saw palmetto extract have been studied for their potential to relieve urinary symptoms associated with BPH, a non-cancerous enlargement of the prostate [10].
A recent double-blind, placebo-controlled study published in BMC Urology (2020) showed that beta-sitosterol-enriched saw palmetto oil significantly improved symptoms of BPH and androgen deficiency compared to conventional saw palmetto oil and placebo [10].
Over 12 weeks, men aged 45 to 65 with mild to moderate BPH who took the enriched supplement had greater reductions in urinary symptoms—measured by the International Prostate Symptom Score—and reported better quality of life. They also had increased testosterone levels without negative effects on PSA levels. These findings suggest that beta-sitosterol-enriched saw palmetto oil may be a more effective natural option for promoting prostate health and easing BPH symptoms [10].
Pygeum Africanum Extract
A comprehensive review evaluated the effectiveness of Pygeum africanum extract in treating BPH symptoms [11]. The review analyzed data from 18 studies involving 1,562 men with BPH.
The findings showed that men taking Pygeum africanum were more than twice as likely to report improvement in overall symptoms compared to those taking a placebo [11].
Specifically, the extract significantly reduced:
- Urinary frequency, including nighttime urination, increased by 19%.
- Peak urine flow rates increased by 23%.
- Residual urine volume decreased by 24%.
The study also noted that Pygeum africanum was generally well-tolerated, with mild and infrequent side effects. These results suggest it may be a beneficial natural therapy for relieving urinary symptoms associated with BPH and improving quality of life [11].
Cranberry Fruit Powder
A notable double-blind, randomized, placebo-controlled study published in the World Journal of Urology examined the effects of a proprietary cranberry fruit powder (Flowens) on urinary symptoms in men over 45 [12].
Over six months, 124 men with mild to moderate urinary symptoms and PSA levels below 2.5 ng/mL took either 500 mg or 250 mg of cranberry powder or a placebo daily.
The results showed that men taking the cranberry supplement had a significant, dose-dependent improvement in urinary symptoms compared to the placebo group. Specifically:
- The International Prostate Symptom Score (IPSS) decreased by 3.1 points in the 250 mg group and 4.1 points in the 500 mg group.
- The placebo group saw a reduction of only 1.5 points.
- Those in the higher-dose cranberry group also had significant improvements in urinary flow rates and bladder emptying.
Importantly, no adverse effects were reported, and there were no significant changes in PSA levels or other safety markers. The study concluded that daily supplementation with cranberry fruit powder effectively and safely reduced urinary symptoms in men, suggesting it as a promising natural therapy for improving prostate health and urinary function [12].
Supporting Prostate Health Naturally
Healthmasters’ Prostate Support supplement contains a combination of beta-sitosterol, saw palmetto extract, Pygeum extract, and Flowens Cranberry Fruit Solids. These natural ingredients have been studied for their potential benefits in promoting prostate health and alleviating urinary symptoms.
Conclusion
The overdiagnosis of prostate cancer is a complex challenge in modern healthcare. PSA screening risks identifying tumors that may never cause harm. The consequences of overdiagnosis are significant—they include physical side effects from unnecessary treatments, emotional distress, and increased healthcare costs.
By focusing on individualized care, using advanced diagnostic tools, and considering natural approaches to support prostate health, we can reduce the burden of overdiagnosis. Empowering patients through shared decision-making ensures that healthcare choices align with personal values and lead to better outcomes.
References:
[1] Schröder FH, Hugosson J, Roobol MJ, et al. Screening and prostate-cancer mortality in a randomized European study. N Engl J Med. 2009;360(13):1320-1328. doi:10.1056/NEJMoa0810084; https://www.nejm.org/doi/full/10.1056/NEJMoa0810084
[2] Andriole GL, Crawford ED, Grubb RL III, et al. Mortality results from a randomized prostate-cancer screening trial. N Engl J Med. 2009;360(13):1310-1319. doi:10.1056/NEJMoa0810696; https://www.nejm.org/doi/full/10.1056/NEJMoa0810696
[3] Andriole GL, Crawford ED, Grubb RL III, et al. Prostate Cancer Screening in the Randomized Prostate, Lung, Colorectal, and Ovarian Cancer Screening Trial: Mortality Results After 13 Years of Follow-up. Journal of the National Cancer Institute. 2012;104(2):125-132. doi:10.1093/jnci/djr500; https://pubmed.ncbi.nlm.nih.gov/22228146/
[4] Hamdy FC, Donovan JL, Lane JA, et al. 10-year outcomes after monitoring, surgery, or radiotherapy for localized prostate cancer. N Engl J Med. 2016;375(15):1415-1424. doi:10.1056/NEJMoa1606220; https://www.nejm.org/doi/10.1056/NEJMoa1606220
[5] Loeb S, Sanda MG, Broyles DL, et al. The prostate health index selectively identifies clinically significant prostate cancer. J Urol. 2015;193(4):1163-1169. doi:10.1016/j.juro.2014.10.121; https://www.auajournals.org/doi/10.1016/j.juro.2014.10.121
[6] Kasivisvanathan V, Rannikko AS, Borghi M, et al. MRI-targeted or standard biopsy for prostate cancer diagnosis. N Engl J Med. 2018;378(19):1767-1777. doi:10.1056/NEJMoa1801993; https://www.nejm.org/doi/10.1056/NEJMoa1801993
[7] Klotz L, Vesprini D, Sethukavalan P, et al. Long-term follow-up of a large active surveillance cohort of patients with prostate cancer. J Clin Oncol. 2015;33(3):272-277. doi:10.1200/JCO.2014.55.1192; https://ascopubs.org/doi/10.1200/JCO.2014.55.1192
[8] Carter HB, Albertsen PC, Barry MJ, et al. Early detection of prostate cancer: AUA guideline. J Urol. 2013;190(2):419-426. doi:10.1016/j.juro.2013.04.119; https://www.auajournals.org/doi/10.1016/j.juro.2013.04.119
[9] U.S. Preventive Services Task Force. Screening for prostate cancer: US Preventive Services Task Force recommendation statement. JAMA. 2018;319(18):1901-1913. doi:10.1001/jama.2018.3710; https://jamanetwork.com/journals/jama/fullarticle/2680553
[10] Sudeep, H.V., Thomas, J.V. & Shyamprasad, K. A double blind, placebo-controlled randomized comparative study on the efficacy of phytosterol-enriched and conventional saw palmetto oil in mitigating benign prostate hyperplasia and androgen deficiency. BMC Urol 20, 86 (2020). doi:10.1186/s12894-020-00648; https://bmcurol.biomedcentral.com/articles/10.1186/s12894-020-00648-9
[11] Ishani A, MacDonald R, Nelson D, et al. Pygeum africanum for benign prostatic hyperplasia. Cochrane Database of Systematic Reviews. 2000;(1):CD001044. doi:10.1002/14651858.CD001044; https://www.cochranelibrary.com/cdsr/doi/10.1002/14651858.CD001044/full
[12] Vidlar A, Student V Jr, Vostalova J, Fromentin E, Roller M, Simanek V, Student V. Cranberry fruit powder (Flowens™) improves lower urinary tract symptoms in men: a double-blind, randomized, placebo-controlled study. World J Urol. 2016 Mar;34(3):419-24. doi: 10.1007/s00345-015-1611-7; https://pubmed.ncbi.nlm.nih.gov/26049866/
*The matters discussed in this article are for informational purposes only and not medical advice. Please consult your healthcare practitioner on the matters discussed herein.
*These statements have not been evaluated by the Food and Drug Administration. Healthmasters' products are not intended to diagnose, treat, cure, or prevent any disease.
